DANVILLE - Decades ago, a day at school for a kindergartener would usually involve an afternoon nap. Today, some schools have phased that out, leaving parents to wonder what’s right.
Luis Garcia, MD, an OSF HealthCare pediatrician, says daytime sleep plays an important role in a child’s development. He says parents should look at it in terms of daytime sleep and nighttime sleep added up to total sleep. He stresses that each child has unique needs, and you should get to know your child’s sleep habits. But there are guidelines. For young kids, Dr. Garcia says nighttime sleep stays mostly consistent at 10 hours. Daytime sleep varies by age.
“Usually, the need for naptime decreases when kids reach 4 to 6 years old,” Dr. Garcia says. “At that point, they only need to sleep the 10 hours at night.”
When and how long
Dr. Garcia says naps for kids should be 30 minutes to two hours. So, you can do some math. For example: your 2-year-old needs four hours of daytime sleep with naps no greater than two hours. So, aim for some two-hour slumbering mid to late morning and early afternoon.
“It’s not recommended to nap after 3 or 4 p.m. to avoid causing disruptions at bedtime,” Dr. Garcia warns. “We want to allow at least four hours between last nap and bedtime to avoid the kids being too tired at bedtime.”
Bad nighttime sleep leads to irritability and poor concentration the next day, he adds.
No more naps
Dr. Garcia suggests parents look for signs that their child is ready to stop napping.
“Is the kid refusing or having a hard time taking a nap? If they do take a nap, do they have a problem falling asleep at night?” Dr. Garcia asks.
You should also talk to your child’s school or day care. If they have daily nap time, let that continue until the child ages out of the facility. If the facility is flexible, inform them of your child’s sleep habits and come up with a plan.
When the time comes to stop naps, Dr. Garcia recommends a clean break. There will likely be some fussiness, but it will subside. Moving bedtime up by 20 to 30 minutes can help.
Sleep tipsSome general good sleep tips:
Make your home’s lighting natural: bright during the day, darker as night approaches and dark at night.
Make the bed the place to sleep. Do other activities like looking at screens in another room, and don’t look at screens right before bedtime.
Get into a routine by going to sleep and waking up at around the same time each day. And make the sleep and wake times normal. Waking up mid-morning each day, while a routine, isn’t the best idea.
Avoid large meals and caffeine before bed.
If you are a light sleeper, use an artificial noise machine.
Why can I speak about this issue? I worked as a pharmacy technician before working as a Registered Nurse (RN) and ultimately becoming a Nurse Practitioner (NP) in 2000. I have been employed in health care for 33 years, including over 20 of those years as a NP. At present, I work in a specialized emergency service, and am attending the University of Washington for a Doctor of Nursing Practice (DNP) degree. I am writing in hopes to affect change on this ubiquitous delivery of health care problem.
A personal story exemplifies this issue. My 90-year-old grandfather was discharged from an ER and resumed taking a long discontinued antihypertensive (blood pressure) medication from an old pill bottle. He took this in addition to his newly prescribed antihypertensive medication, both medications listed as active in his discharge instructions.
Fortunately, my grandfather was okay, and my mother caught this error and understandably had something to say about it. She drove back to the hospital to give them a piece of her mind, before recommending they come up with a better system. They agreed.
One recurring and nationwide theme are health care providers, and patients, becoming confused with the list of medications in their medical records in all phases of care, including at hospital admission and discharge. This medication list often includes medications that are listed as active and those they haven't taken at times since many years ago.
Sadly, this is not an exaggeration, and often leads to harmful medication errors which are a big problem during all phases of health care. Affected phases include outpatient ambulatory care clinics, during hospital admissions, during hospital stays and hospital discharge. Because of these gaps, medication errors are not surprisingly a leading cause of injury or death.
This is a serious issue that I believe can be solved with a concerted effort by an interdisciplinary team approach along with a streamlined electronic health record system. This is in addition to an emphasis on patient education throughout all stages of treatment which includes outpatient care, an urgent hospital visit or inpatient stay. Providers and ancillary services should always be involved in this process.
Better practice solutions:
1. For health care providers, at all phases of treatment, if it remains unclear if a patient is taking a medication, ask questions, and if medication reconciliation is not possible then list it as such. Increasing awareness of this problem in the advent of increasing use of Electronic Health Records (EHR) is key.
2. Incorporation of admission and discharge medication reconciliation as a continuous process by admitting and discharging RNs, the pharmacist and nurse practitioner and physicians.
As noted by J AM Med inform Association (2016) working towards a solution would include incorporating reconciliation modules that are interoperable with other Electronic Health Record components. This includes medication history, the computerized order set and discharge documentation. Some EHRs have some interoperability with external sources (hospitals, clinics, pharmacy) to import medication history and share updated medication list at discharge, although this is not fail safe and should not be relied on itself alone.
3. As health care consumers, don't be afraid to ask questions or clarification. Most health care providers want you to be involved in your own care. You reserve this right 100 percent and it is okay to ask questions and include your loved ones to advocate for you in your treatment plan.
In summary, medication confusion and errors are fear reaching. It is up to us as health care providers to be conscientious and provide essential emphasis on patient education and collaboration. Encouraging patients and their loved ones to actively participate in their care is vital. This includes asking questions and seeking clarification about medications along with interdisciplinary providers to help prevent confusion and potential medication errors. Involving patient's loved ones can contribute to healthy outcomes. Refining EHR is of the utmost importance.
I thank all health care providers for dedication to this important cause, and I wish success in your continued efforts to make a positive impact on health care practices while encouraging health consumers to be proactive in their care.
Angela Buxton, FNP-BC is a national Board-Certified (BC) Family Nurse Practitioner (FNP) since 2000 and who is originally from Massachusetts, obtaining her undergraduate and graduate degrees at UMASS, Amherst, and worked as both a Registered Nurse (RN) and FNP throughout her career. She is currently attending the University of Washington to expand her skills as a Doctor of Nursing Practice in Psychiatric Mental Health. She has now been working as a NP at Harborview Medical Center in Seattle, Washington for the last 20 years. She enjoys her role in assessing, diagnosing and developing client centered treatment plans, not limited to prescribing medications. Population includes those who are underserved and across the lifespan. She has membership in Snohomish County, WA Search and Rescue (SSAR), has participated in team endurance events with lessons learned that crossover into daily life. Other outside interests include photography, painting, skiing and hiking the Pacific Northwest.
GODFREY - The 2015 horror film “The Visit” gives the Hollywood treatment to sundowning. An impostor grandmother is seen running the halls, scratching the walls and vomiting, terrorizing two children in the home.
A little exaggerated, says Courtney McFarlin, PA, an OSF HealthCare internal medicine provider who specializes in geriatrics. But she says sundowning is an all too real experience for some older adults.
What is sundowning?
McFarlin explains that sundowning is not a medical condition, but rather a way to describe behavior seen at night. It’s triggered by a disruption in your circadian rhythm.
“That’s our body’s natural, 24-hour sleep/wake cycle,” McFarlin says. “It’s regulated by the hypothalamus in the brain. Based on daylight and darkness, it tells our body to be alert during the day. And it helps us settle down in the evening to want to go to sleep.”
Key takeaways:
Sundowning describes nighttime behavior in older adults, especially those with dementia, due to a disruption in the circadian rhythm. The person may be agitated, moody, not want to go to sleep or physically aggressive.
Ways to help include medicine like melatonin, eliminating long naps and practicing general good sleep hygiene. Homes should also be arranged so the elder does not fall or wander outside.
A caregiver may ultimately have to decide whether to move the person to an assisted living facility.
Many things can disrupt your circadian rhythm, like illness, stress, artificial light and genetic factors. But McFarlin says sundowning is most often seen in older adults with dementia and similar disorders like Parkinson’s disease and Huntington’s disease. Chronic alcohol use can also bring about sundowning.
What does sundowning look like? McFarlin says the person may be agitated, have mood changes and pace around. They may not want to go to sleep. And the person may even physically lash out at others.
“Reports and research have shown that it’s most common when people are in mild or moderate stages [of dementia],” McFarlin says. “You would think as one progresses with dementia, it would get worse. But it actually improves a little bit.”
How to help
McFarlin says caregivers of older adults often come to her with a plea: help us do something about my loved one’s nighttime behavior. The caregivers are sometimes awake through the night keeping an eye on things, leading to sluggishness, crankiness and other issues during their workday.
First, McFarlin reminds you that support groups exist – if not in-person in your community, then online – for caregivers of older adults. But for medicinal aids, McFarlin says melatonin is a good first option.
“It’s a natural hormone that our body produces that helps aid in sleep,” she says.
McFarlin adds that studies have found decreased levels of melatonin in older adults with or without dementia.
Serotonin-based medications, hypnotics and anti-anxiety medications can also help. Paxil, Prozac, Seroquel, Risperdal and Haldol are common brand names. Talk to your health care provider or a sleep specialist if you have questions about these medicines.
Something to strike from your loved one’s routine: long naps.
“It’s suggested that a less than three-hour naptime schedule is advised,” McFarlin says. “If I find my patients are napping quite a bit, I’ll encourage them to take less naps.”
Other sleep hygiene tips:
Make your home’s lighting natural: bright during the day, darker as night approaches and dark at night.
Make the bed the place to sleep. Do other activities like looking at screens in another room, and don’t look at screens right before bedtime.
Get into a routine by going to sleep and waking up at around the same time each day. And make the sleep and wake times normal, as if the older adult was going to work. Waking up mid-morning each day, while a routine, isn’t the best idea.
Avoid large meals, caffeine and alcohol before bed. McFarlin says lunch should be the biggest meal.
Stay busy during the day so you feel tired at night. Regular exercise can help with this.
If you are a light sleeper, use an artificial noise machine.
Since people with sundowning behaviors can pace and wander, make sure your home is trip-proof and escape-proof. Rugs, chairs and nightstands should be moved or removed. McFarlin says providers can also recommend physical therapy or devices like a walker, wheelchair or bed alarm.
“[People can] actually unlock the door and wander outside in the middle of the night,” McFarlin warns. “So, make sure the door is properly locked. If the adult is someone who wanders at night, make sure they don’t have the ability to leave home.”
Ultimately, you may have to decide whether a different living arrangement is best for your loved one.
“That could be remaining at home and more family coming in. Because that’s our first choice – to leave the person at home as long as they can,” McFarlin says.
“But when it becomes unsafe for the person or exhausting the caregiver, it’s my responsibility to engage other options,” like an assisted living facility, she says.
PONTIAC - People everywhere are conquering their cabin fever and are enjoying the great outdoors after a long, bitter winter. But before you head out for that hike, health care experts remind you to take precautions to avoid tick bites. Read more . . .
CHICAGO - An Illinois law professor is weighing in on what she called a "very public and open test of due process" for immigrants being deported from the United States without court hearings. Read more . . .
CHAMPAIGN - In a show of solidarity against President Donald Trump's trade and immigration policies, which critics say are harming families and retirement savings, more than a thousand protesters gathered Saturday at West Park near downtown Champaign for the Hands-Off! Mobilization rally. Read more . . .
Photo Galleries
A couple of runners found themselves in the wrong race at this year's Illinois Marathon. Over 60 photos from the race that you should see.


 by Tim Ditman
by Tim Ditman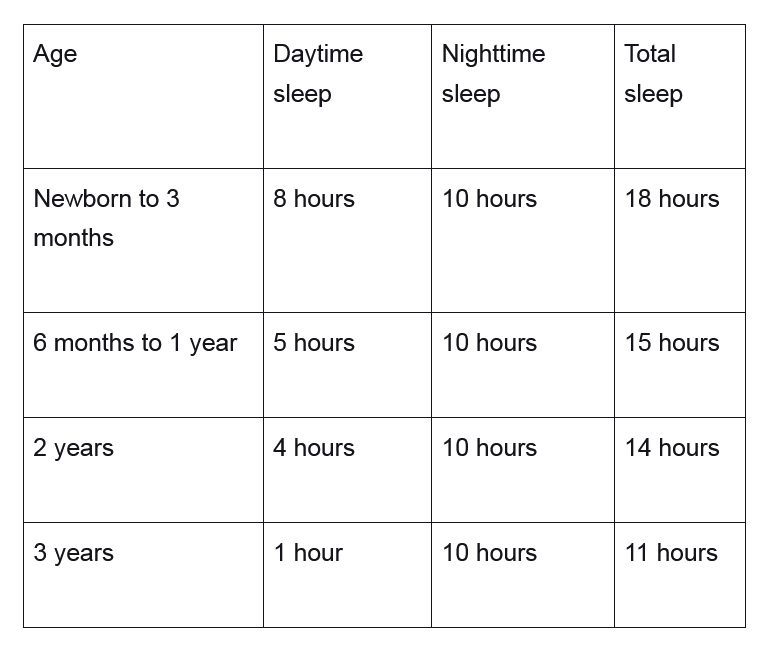 “Usually, the need for naptime decreases when kids reach 4 to 6 years old,” Dr. Garcia says. “At that point, they only need to sleep the 10 hours at night.”
When and how long
Dr. Garcia says naps for kids should be 30 minutes to two hours. So, you can do some math. For example: your 2-year-old needs four hours of daytime sleep with naps no greater than two hours. So, aim for some two-hour slumbering mid to late morning and early afternoon.
“It’s not recommended to nap after 3 or 4 p.m. to avoid causing disruptions at bedtime,” Dr. Garcia warns. “We want to allow at least four hours between last nap and bedtime to avoid the kids being too tired at bedtime.”
Bad nighttime sleep leads to irritability and poor concentration the next day, he adds.
No more naps
Dr. Garcia suggests parents look for signs that their child is ready to stop napping.
“Is the kid refusing or having a hard time taking a nap? If they do take a nap, do they have a problem falling asleep at night?” Dr. Garcia asks.
You should also talk to your child’s school or day care. If they have daily nap time, let that continue until the child ages out of the facility. If the facility is flexible, inform them of your child’s sleep habits and come up with a plan.
When the time comes to stop naps, Dr. Garcia recommends a clean break. There will likely be some fussiness, but it will subside. Moving bedtime up by 20 to 30 minutes can help.
Sleep tips
Some general good sleep tips:
“Usually, the need for naptime decreases when kids reach 4 to 6 years old,” Dr. Garcia says. “At that point, they only need to sleep the 10 hours at night.”
When and how long
Dr. Garcia says naps for kids should be 30 minutes to two hours. So, you can do some math. For example: your 2-year-old needs four hours of daytime sleep with naps no greater than two hours. So, aim for some two-hour slumbering mid to late morning and early afternoon.
“It’s not recommended to nap after 3 or 4 p.m. to avoid causing disruptions at bedtime,” Dr. Garcia warns. “We want to allow at least four hours between last nap and bedtime to avoid the kids being too tired at bedtime.”
Bad nighttime sleep leads to irritability and poor concentration the next day, he adds.
No more naps
Dr. Garcia suggests parents look for signs that their child is ready to stop napping.
“Is the kid refusing or having a hard time taking a nap? If they do take a nap, do they have a problem falling asleep at night?” Dr. Garcia asks.
You should also talk to your child’s school or day care. If they have daily nap time, let that continue until the child ages out of the facility. If the facility is flexible, inform them of your child’s sleep habits and come up with a plan.
When the time comes to stop naps, Dr. Garcia recommends a clean break. There will likely be some fussiness, but it will subside. Moving bedtime up by 20 to 30 minutes can help.
Sleep tips
Some general good sleep tips:








